The best age is between 11 and 13 years. Before the age of 11 the bone, especially in the maxilla, may be too thin or the density may be too low, which reduces the mechanical retention of the screws. The strength of the bone increases with age.
However, with age the interdigitation of the sutures and resistance against separation increase. That’s why it is recommended to start the orthopedic treatment before the age of 13, especially in girls. However, a great interindividual variability in growth changes is observed. That’s why a limited growth stimulation can still occur after the age of 13.
Besides stimulation of suture growth, modelling at the ramus and at the glenoid fossa results in a closure of the gonial angle and a slight posterior repositioning of the articulation. This restrains the forward projection of the bony chin. It is not clear yet if these modelling changes last longer than growth changes in the sutures. About 40% of the overall antero-posterior changes are in the mandible.
Delayed eruption of the lower canines may complicate the insertion of the mandibular plates. This is further discussed in the “Surgeon” section.
The elastic traction is started about 2 weeks after the placement of the miniplates. The initial force should be low and gradually increased over the first 4 months by reducing the diameter of the elastics. The force depends on the distance between the upper and lower anchors. However, a typical sequence of light elastics is as follows:
![]()
The initial force is about 100 grams each side and the final force after 4 months should be about 175 grams each side with a maximum force level of 200 grams. This loading is maintained for the rest of the treatment. Higher force levels do not result in more protraction of the midface.
The patient has to renew the elastics at least every morning and evening. The instructions how to apply the elastics are given in the Patient Section. The patient has to wear the elastics 24 hours a day and should not remove them for eating or during sleeping.
There is no evidence that Rapid Maxillary Expansion (RME) or Alternate Rapid Maxillary Expansion and Constriction (Alt-RAMEC) significantly increase the amount of protraction of the midface. ‘Disarticulation’ of the sutures seems not to have a major effect on the forward growth of the maxilla. However, during the expansion the infra-orbital bone surface is slightly moved forward and towards the outside, resulting in a slight forward movement of point A.
Mild transverse discrepancies are corrected spontaneously during the bone anchored class III traction thanks to the improvement of the antero-posterior relation between upper and lower jaw, and don’t need any expansion of the maxilla.


RME may be indicated in cases with a severe transverse hypoplasia of the maxilla, resulting in a unilateral or bilateral crossbite. Expansion should be done before starting the orthopedic treatment.




In cases with an anterior crossbite without open bite, the forward movement of the upper arch will be restrained by the lower incisors. Then a biteraiser is needed.

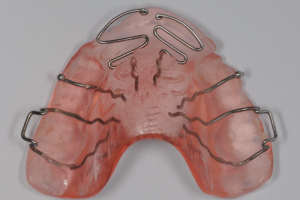
Bonded acrylic bite raisers have the advantage that no compliance is needed. However, a removable acrylic bite plate has the advantage that springs can be added to procline one or more incisors, to cross the bite quicker, and to reduce the wearing time of the appliance. Grinding of the teeth always results in indentations of the lower teeth into the acrylic covering the upper teeth. These indentations restrict the antero-posterior growth changes. That’s why you should remove these indentations at each monthly visit by grinding the acrylic. This is much easier on a removable appliance than on a bonded bite raiser in the mouth.
To avoid time consuming adjustments of the acrylic at the first visit, together with the upper and lower alginate impression or digital scan, you should send to your lab technician a waxbite or digital registration with the incisors end to end, so that he can make the appliance with the appropriate thickness. For the adam and ball clasps we recommend 0.7mm Spring Hard Stainless steel wire from Dentaurum. Rather than using 4 separate propulsion springs you better use double springs also in 0.7mm wire. The acrylic covering the propulsion springs can be reinforced by a metal grid.
Due to a trauma, a hook from the lower Bollard may fracture. You can easily make a new hook by inserting a piece of .016”x.022” stainless steel wire into the .018”x.025” tube of the Bollard. It can be secured by bending the outcoming end down and inwards. If there is a risk of irritation of the lip, after bending, the end can be covered by a drop of flowable composite.
Sometimes an elastic fixed between the upper and lower Bollard miniplate may irritate the gums or touch a tooth. This can be solved by adding a hook into the lower Bollard tube to bring the point of force application to a higher level , away from the tooth or the gums.



The active treatment consists in wearing the intermaxillary elastics during at least 1 year. In cleft patients a wearing time of 18 months is recommended.
Thereafter a treatment with fixed appliance is commonly needed to straighten the arches and to obtain a good stable occlusion. During this treatment the elastic traction is usually interrupted because of interference between the elastics and the fixed appliance. If not, elastic traction can further be continued.
After debonding the fixed appliance, there still is a remaining growth potential which may result in some relapse of the skeletal class III. In this case additional elastics should be worn for 24 hours a day as long as the relapse tendency persists. That’s why it is recommended to remove the bone anchors only close to the end of growth.
Asymmetrical growth of the mandible results in a deviation of the chin and the lower dental midline.
Modelling processes in the ramus and the gonial angle are affected by continuous bone supported elastic traction. Asymmetrical traction may result in asymmetrical modelling at the left and right ramus and in both glenoid fossa’s, but also causes asymmetrical orthopedic effects in the maxilla. Clinical observations show that the growth changes in the upper jaw mostly happen in the first 6 months. In order to avoid asymmetries in the upper jaw it is recommended to start the elastic traction on both sides and only after 6 months to switch to unilateral elastic use for the rest of treatment in cases with an asymmetry of the mandibula.


1.The anchorage: with a facemask the elastics are fixed to a bonded or removable acrylic splint or a hyrax in the upper jaw. If skeletal anchorage is used in the maxilla, a double amount of protraction is obtained, not only with the BAMP protocol but also with a facemask. The key for successful midface protraction is in the first place the use of skeletal anchorage instead of a dento-alveolar support.
2.The force: with bone anchored orthopedics half of the force is used compared with facemask. Higher force levels do not result in more protraction. Furthermore, with BAMP the elastic traction is continuous and is not interrupted during the day.
3.The age: while it is recommended to start facemask treatment in early mixed dentition (before the age of 9), the BAMP protocol is started in the late mixed dentition (between 11 and 13 years).
4.Intra-oral appliance: because no extra-oral appliance is needed, compliance for wearing the elastics is better with BAMP than with facemask and elastics can be worn 24 hours a day.
5.Expansion: expansion before facemask still is the golden standard. However, with skeletal anchorage no expansion is needed, except with a severe transverse hypoplasia.
6.Mandibular rotation: pressure from the chin cup of the facemask always results in a posterior rotation of the mandible and an increase of the vertical dimension of the face. With BAMP the line of force from the elastics is above the condyles and results in an anterior rotation of the mandible and a slight closure of the mandibular plane angle.
Scar tissues from the surgical closure of the lip, hard, and soft palate result in a restriction of the forward growth of the maxilla and a hypoplasia of the midface. Recent research shows that despite the presence of scar tissues, in cleft patients a very similar outcome can be obtained with BAMP compared with non-cleft patients, also in the maxilla. However, it is recommended to wear the elastics for at least 18 months.
Mobility can be caused by bad oral hygiene and local infection, jiggling forces, or poor bone quality, especially in the upper jaw where the cortical bone can be very thin in growing patients. If the mobility persists, the bone anchor should be removed under local anaesthesia.
Two to three months later the bone will be healed and of better quality than at the first surgery, so that the miniplate can be replaced, with reduced risk of loosening.
India, Hubli
Third International Orthodontic Symposiu
Germany, Ulm
Congress of German Orthodontic Society (DGKFO)
Japan, Yokohama
Congress of the World Federation of Orthodontists (WHO)
Italy, Florence
Congress of the Italian association of orthodontists (SIDO)
Belgium, Bruges
 Bollardcourse 2020
Bollardcourse 2020